
Pre-admission clinic
You will be asked to attend a pre-admission clinic before your operation. This is to discuss your past medical history and assess your fitness for anaesthesia. It also allows the hospital to prepare for your surgery and ensure your operation goes as smoothly as possible. It is also a chance for you to ask any questions you may have and alleviate any concerns prior to the surgery.
Please note that neither the surgery nor any other treatment will be done without your agreement (consent). It is your right to refuse treatment at any time, or until you have enough information to feel comfortable about giving your consent.
What are the risks?
All operations involve an element of risk. We do not wish to over-emphasise them but feel that you should be aware of them before and after your operation. Please discuss these issues with the doctors if you would like further information. The risks include:
- Complications relating to the anaesthetic such as sickness, nausea or rarely cardiac, respiratory or neurological (less than 1% each, i.e. less than one person out of one hundred)
- Infection. These are usually superficial wound problems. Occasionally deep infection may occur many months after the operation (less than 1%)
- Deep vein thrombosis (less than 1%)
- Bruising/bleeding
- Persistent pain in/around the knee joint (less than 5%)
- Damage to the nerves and blood vessels around the knee (less than 1%)
- Recurrence of instability within the knee joint
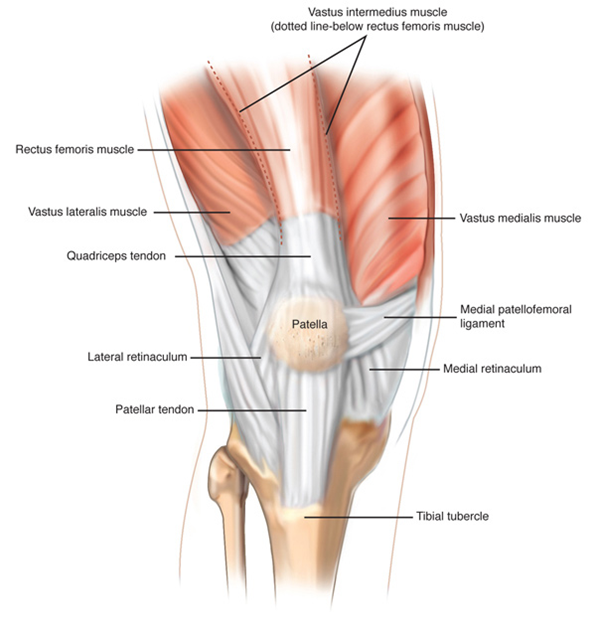
Medial Patello-Femoral Ligament (MPFL) Reconstruction
What is it?
The medial patella-femoral ligament (MFPL) is the main stabiliser for the inside edge (medial) of the patella (knee cap). This ligament prevents the patella from dislocation to the outer (lateral) side of the knee. With any lateral displacement of the patella the MPFL can be injured or torn, leading to recurrent dislocations or partial dislocation (subluxation). Repair of the MPFL is a surgical reconstruction to return to the patella as close as possible to its normal state within the knee.
Right knee
The Procedure
The operation is done under a general anaesthetic (when you are asleep) to allow you to fully relax. It is done by using a minimally invasive technique which means scarring and the risk of infection is as less as possible.
Five small incisions (cuts) are made around the knee to access the joint and a small portion of the hamstring is then passed through small drill holes in the knee cap. The other end is then inserted it into the inner aspect of the thigh bone using a plastic screw to hold it in place. This stabilises the movement of the knee cap.
The procedure takes around one hour.
(Note: picture is the left knee)

Benefits of Surgery
Success rates are high in terms of improving function and reducing instability of the patella:
- Improved knee stability with reduced chance of patella dislocation
- Improved function/mobility
- Reduced pain
- It may take up to 12 months for a full recovery and return to sport
Some people will have persisting symptoms depending on the anatomy of their knee joint, any damage already done to the bone surface and how well they engage with their post op rehabilitation in Physiotherapy.
Managing your pain
It is likely that your pain will be well controlled immediately post-operative as local anaesthetic is usually placed into the joint during the procedure . It is therefore sensible to take some regular pain relief so that when the local anaesthetic wears off you remain comfortable. It is important your pain is under control before you leave hospital.
Should you experience any increase in pain and swelling not relieved by elevation and rest, or any pain in the calf, please consult your GP.
Ice
Ice can be very useful to help manage swelling and pain. You need to be careful with it’s use to ensure you do not damage your skin. We suggest you follow the precautions below:
- You should ensure that the area to be treated is sensitive to temperature by placing a cold and then a warm object against it and making sure you can tell the difference
- Use crushed ice, gel packs or frozen peas as an ice pack but always ensure that there are two layers of towel between your skin and the ice pack
- Check your skin after 10 minutes, it is likely to be red but should not be white or blue. If you are concerned then remove the ice pack immediately. If your skin is frail or you have poor circulation you should check after five minutes. If there is no adverse reaction then the pack can be applied for a total of 20 minutes
Ice packs are most effective when applied for 10-20 minutes every three-four hours.
If you feel pain at any stage, always remove the ice pack and check the skin for signs of loss of circulation e.g. white/purple/blue or very cold skin. Ice packs used incorrectly can cause ice burns.
Swelling
Your knee may swell for a couple of months or even longer after the surgery. It is normal to have occasional swelling for up to a year. This is a normal part of healing but if it becomes excessive this can lead to increased pain and slower return to activities. To prevent this, sit with your foot elevated higher than your hip whenever possible and pace your activities.
If at any time you notice any discharge, smell, irritation, or redness around the wounds/dressings, you must contact your GP as this could be a sign of an infection.
Mobility
You are able to mobilise fully weight bearing as tolerated unless told otherwise. This means you can put as much weight through the leg as you are able to following your surgery. This will help the healing process . You will need to walk with crutches initially whilst you are recovering to make sure you have a correct walking pattern and help your balance. Once you have a good walking pattern you can discard the crutches and your Physiotherapist will guide you on this.
You will be able to leave hospital when you can bend your knee 90° and completely straighten your knee. The Physiotherapist on the ward will help you with this, and make sure you are safe mobilising including on the stairs before discharge.
Questions we are often asked
The operation is carried out under general anaesthetic, and you can normally go home the day after surgery.
Following the surgery a large padded bandage will be applied. You should keep this bandage dry and leave it undisturbed until your clinic appointment in two week times. This is where your wound will be reviewed and sutures removed.
Although you will only have small scars, this procedure can be painful due to the surgery performed inside your knee. Although the operation is to relieve pain, it may be several weeks until you begin to feel the benefit. It is important that you keep the pain under control with regular pain relief medication. We do not want you to mask the pain but you must be able to feel comfortable. This will allow you to sleep better, complete the exercises and therefore allow the operation to be as successful as possible.
A prescription for continued pain relief medication may be given to you for your discharge home. If you require further medication after these are finished, please contact your general practitioner (GP).
No. You are normally allowed to mobilise fully weight bearing without a brace after the surgery. Your consultant or Physiotherapist on the ward will inform you otherwise if there are any specific restrictions.
Your stitches will need to be removed after 10—14 days. This is usually done at your first clinic appointment after the operation.
Keep the wound dry until it is healed. Protect the wound with cling film or plastic bag when washing. If you need to change the dressing take care not to disturb the stitches or pad underneath the dressing. Avoid using moisturisers, talcum powder or perfumes near or on the wound.
You need to have a good walking pattern and knee control before you get rid of the crutches. This is usually between three– six weeks after the surgery. Your Physiotherapist will advise you when to begin walking without them. It is important to maintain a good walking pattern so you don’t develop a limp or secondary muscle compensations by coming off the crutches too soon.
You will be seen be a Physiotherapist within two weeks after your operation. This delay allows the discomfort from the operation to reduce and the healing process to be well under way. This will be arranged by the Physiotherapist on the ward. If you would prefer to be seen at a Physiotherapy Department local to you please let the ward Physiotherapist know.
You have to come back to the Orthopaedic Clinic two weeks after your surgery. This is so your stitches can be removed and your wound reviewed. Future appointments are made after this as required.
Exercises
It is important to start exercising soon after your surgery to regain movement, strength and balance. This exercise programme should be carried out four to six times throughout the day. The strength to the quadriceps (thigh muscle) is vital to knee stability and prevention of further injury. It is important to do the exercises slow and controlled rather than quick movements. Initially they may be uncomfortable but it is important not to push into pain.
Point your toes downwards then pull your foot up. Repeat 20 times.

Sitting in a chair or lying on your back, bend and straighten your knee, sliding your heel back wards. Repeat 10 times.

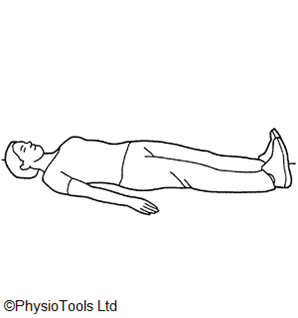
Lying on your back with your knee straight. Bend your ankles towards and push your knees down firmly against the bed. Hold for five secs– relax. Repeat 10 times.
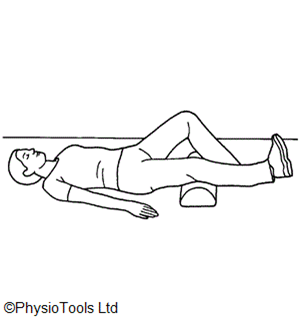
Lying on your back, put a pillow or rolled towel underneath your operated knee. Tighten your thigh mus cle and lift your heel off the floor. Hold approx. five secs and slowly relax. Repeat 10 times.
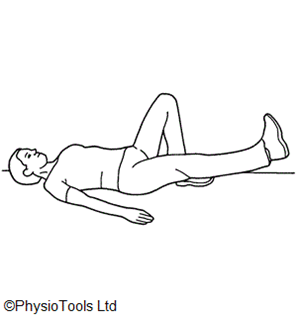
Lying on your back, on your operated leg pull your toes up, straightening the knee and lifting the leg 20cm off the bed. Hold approx. five secs and slowly relax. Repeat 10 times.
Returning to normal activities
Driving
There is no set criteria for driving. You need to ensure you have full control of the car and able to perform an emergency stop. This is roughly between four to six weeks after surgery. Check with your Physiotherapist or Doctor for further advice.
Work
Your return to work will depend on your job. Please discuss this with your Doctor or Physiotherapist.
Sport
You can commence light jogging after three months, with a return to sport between four to six months depending on your sport and level you play at. Your Physiotherapist will guide you through sport specific training should you require it.
Travelling
We advise you refrain from flying for at least six weeks after surgery.
Contact details
Therapy Department
01935 384358
Orthopaedic Outpatient Clinic
01935 384319
16-17-24
Review 06/19


