
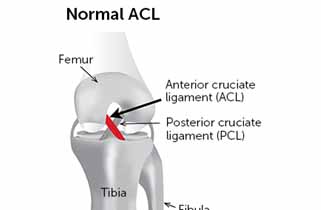
What is the ACL?
The Anterior Cruciate Ligament (ACL) is a thick, broad band which helps to limit the forward sliding movement of the tibia (shin bone) in relation to the femur (thigh bone). It also provides rotational stability. As it is located within the joint capsule, it is common for a lot of swelling to occur when the ligament is damaged. This is due to bleeding.
The ACL is commonly damaged during twisting injuries. Other mechanisms of injury include a sudden deceleration combined with a rotational force (e.g. running & changing direction, landing from a jump or pivoting). Quick and excessive bending (hyper-flexion) or straightening (hyper-extension) type-injuries may also damage the ACL.
Muscle strength provides a very important role in stabilising the knee joint. These muscles include the quadriceps (front of the thigh), hamstrings (back of the thigh) and gastrocnemius (calf). Good strength in your gluteal (buttock) muscles is also vital to aid stability around the knee.
What is an ACL reconstruction?
An arthroscopy surgery is used to repair the ACL. This is an operation to examine the knee joint under anaesthetic. A small incision is made so an instrument, called an arthroscope (a long thin telescope with a video camera), can be inserted into the knee. The surgeon will examine the joint by looking at images sent by the arthroscope to a computer screen and repair damaged structures as necessary.
This allows the surgeon to fully assess the inside of the knee joint including the knee cap (patella), the ligaments (e.g. cruciates or ACL & PCL) the cartilages (menisci or meniscus), and the joint surfaces/lining. A second (and sometimes third) incision is made which allows small instruments to be inserted into the knee to assist with the repair.
The benefit of operating through small incisions like this is that there is minimal disruption to the surrounding tissues allowing you to progress quickly with rehabilitation and return to normal function as rapidly as possible.
The ACL is usually repaired by a graft; commonly taken from your hamstring (muscle at the back of your thigh) or patella tendon (tendon below your knee cap at the front). This graft is secured in place of the damaged ACL, to act as a substitute. Each graft can incur different indications and complications. Your surgeon will discuss this with you, along with which graft is planned to be used.
The surgery is generally performed under general anaesthetic and takes approximately an hour.
This leaflet will help to explain what
you can do to ensure that you have a good recovery and minimise complications.
It will also help you understand what to expect and what is normal after an ACL
reconstruction. A member of the physiotherapy team will generally see you prior
to your surgery to provide advice, exercises and to issue you with crutches.
Immediately after Theatre
You can start your exercises as soon as you remember to when you return from theatre, you will find them in this booklet. Your knee will be wrapped in a thick bandage but you should try to start moving your knee as much as the bandage allows. Staff will help you to get up with the crutches when you have recovered sufficiently from the anaesthetic.
Before you are discharged you will be given specific advice about your wound care and pain relief. The leaflet contains general information about this.
Wound care
The small wounds from the surgery will usually be closed with stitches. These are covered with a dressing and your knee is then wrapped in a layer of cotton wool and a crepe bandage. Discuss with your nurse any queries regarding your wound.
48 hours after the surgery you should remove the crepe bandage and cotton wool layer (unless specified otherwise). Do not disturb the see through dressings and make sure that you keep them clean and dry. You will be seen within two weeks for removal of stitches and your first post-operative check.
It is advised that you keep your wound dry and clean following the surgery. A strip wash is recommended, or you can wrap your leg in cellophane if you want to shower.
If at any time you notice any discharge, smell, irritation, or redness around the wounds/dressings, you must contact your GP.
Managing your pain
It is likely that your pain will be well controlled immediately post operatively as local anaesthetic is usually placed into the joint during the procedure. It is therefore sensible to take some regular pain relief so that when the local anaesthetic wears off you remain comfortable. It is normal to require regular pain relief within the first few weeks after your surgery.
Should you experience any increase in pain and swelling not relieved by elevation and rest, or any pain in the calf, please consult your GP.
Managing swelling
Swelling of the knee is part of the natural healing process but if it becomes excessive this can lead to increased pain, increased time for wound healing, general discomfort and slower return to activities.
Swelling naturally peaks at 3-5 days following an injury or surgery. It is strongly affected by gravity and so if you spend a lot of time on your feet then it is likely to increase as a result. Please follow the advice below to aid your recovery:
- Gravity can be used in our favour by elevating the affected limb. We therefore suggest that you pace your activity, especially over the first week after surgery.
- Rest regularly – do not walk or stand for long periods. Aim for short periods of activity. (Complete rest is also not advised as this can lead to the joint becoming stiff).
- Try to keep your leg up whenever you sit and try to rest your leg in a position where your knee is higher than your hip for short periods through the day.
- Do not rest with a pillow under your knee. This discourages full extension of the knee, which is essential for recovery.
- Keep your compression bandage on for the first 48 hours after your surgery.
- Ice your knee regularly – see overleaf for advice.
Using crutches
You will be issued with and taught to use crutches by a member of the physiotherapy team, usually before your operation. Normally you will place the crutches forward first, followed by the operated leg and then the un-operated one. The nursing staff will ensure you are walking safely with your crutches before you are discharged.
As a general guide you only need to use the crutches for comfort and to prevent you limping. If you decide you only need to use one crutch we advise that you use the one on the side away from the operated leg to keep you well balanced. You should only move on from 2 crutches to 1 crutch or 1 crutch to no crutches when you are able to do so without limping.
Rarely, the surgeon may ask for you to limit the amount of weight on your operated leg. If this is the case then you will be informed of this and given further instruction if needed. It is very important that you follow this advice if it applies to you.
When going upstairs we suggest that you take one step at a time lead with the UNOPERATED (strong) leg. Follow with the OPERATED leg and the crutch, one step at a time. When going downstairs place the crutch(es) on the step below, followed by the OPERATED leg before bringing down the UNOPERATED (strong) leg to join it.
Always use a hand rail or bannister, if there is one available, during your recovery.
Exercises
It is important to start exercising soon after your surgery to ensure that you return to normal movement, strength and activities as soon as possible. After your injury the muscles surrounding the knee would have become weak. The strength of the thigh muscle (the quadriceps) is vital to knee stability and reduce risk of further injury. It is important to perform the following exercises 4-6 times per day. We suggest that you exercise little and often throughout the day. Slow controlled exercises are more effective and more comfortable than quick movements. You may experience some discomfort initially with these exercises but it is important not to push into pain. If your pain persists please contact your GP or physiotherapist.
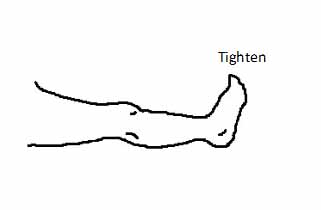
1. In sitting or lying with your leg supported, tighten thigh muscles and straighten the knee as far as you can. Repeat 10 times.
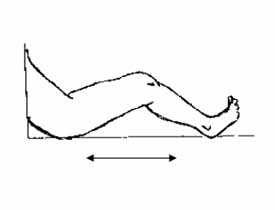
2. Sit or lie with your legs out straight. Gently and slowly slide your heel towards your bottom until it feels tight, then slowly straighten your leg. Do this as pain allows. As your knee bend gets easier you can practice bending your knee while sitting in a chair. Repeat 10 times.
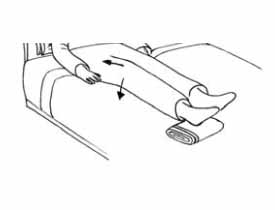
3. Rest your ankle on a small rolled-up towel and let your knee rest into a straight position. To get even straighter, tighten your thigh muscle and push the back of the knee towards the bed. Repeat 10 times.
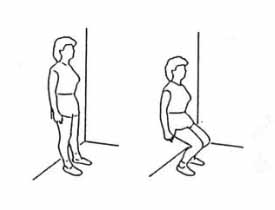
4. Keeping weight evenly distributed between both legs, gently bend both knees a little way as comfort allows and then push up tall again. These exercises help to strengthen the thighs. Some people will find them easier to do while leaning against a wall or holding a work surface. Repeat 10 times.
Returning to normal activities:
Driving
People normally return to driving 4-6 weeks after their surgery. You can drive when you feel safe to perform an emergency stop. It is advisable to inform your insurance company that you have had a knee surgery. If in doubt, liaise with your consultant, physiotherapist or GP.
Work
Your return to work will depend on your job. Please discuss this with your doctor or physiotherapist.
Sport
Your return to sport will depend on the type of activity and the level you play at. Please discuss with your Physiotherapist what sports you can do and when. Earliest return to team or contact sports is approximately 9 months.
Travelling
We advise you to refrain from flying for at least 6 weeks after surgery.
Contact details
If you have a query about exercises or movements, or have not seen a Physiotherapist before being discharged home please contact: Yeovil District Hospital Therapy Department on 01935 384358
Ref:34/20/04
Review: 10/22


